
/
September 3, 2024
Funding cuts from pro-choice groups are affecting abortion access at the same time that clinics are seeing more patients in need of expensive procedures not covered by insurance.
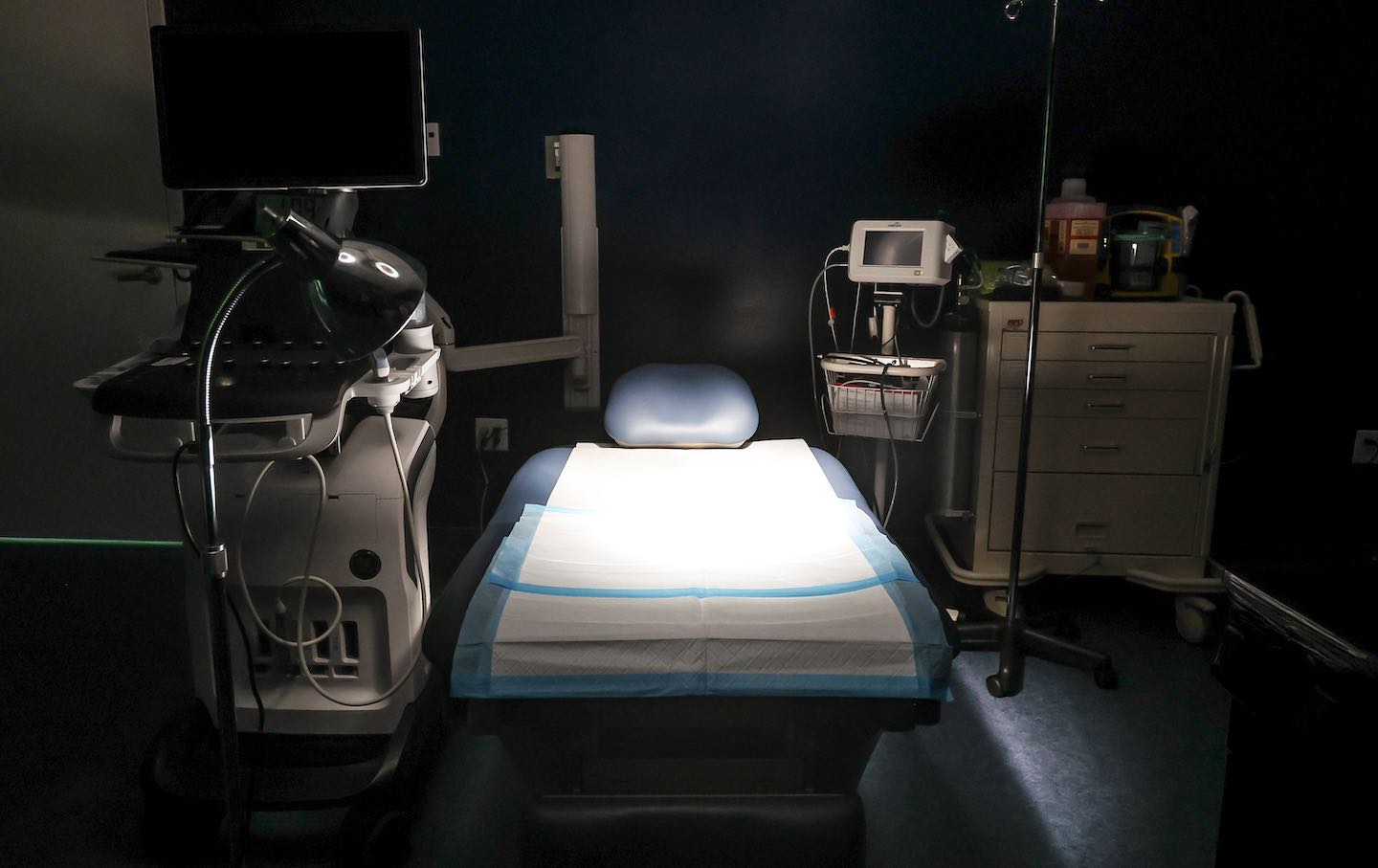
A procedural abortion room at Equity Clinic in Champaign on May 21, 2023.
(Shanna Madison / Chicago Tribune)
Case managers at the DC Abortion Fund never ask callers why they need an abortion. But in recent weeks, some women have been disclosing that they received a diagnosis of a fetal anomaly or that the pregnancy puts their health at risk. To Alisha Dingus, DCAF’s development director, this is a clear sign that people have contacted multiple funds in desperation, only to hear they’ve already hit their budget.
Abortion funds have been struggling in the face of cuts to patient grants from national pro-choice groups that took effect in July, and the crunch comes at the same time that more people need procedures later in pregnancy that cost tens of thousands of dollars, not including travel.
“There’s this pressure being put on callers who are already in a really difficult situation to overshare their medical information because they know it might help them get an extra $1,000 or $2,000,” Dingus said.
Karishma Oza, director of care coordination at DuPont Clinic, an all-trimester provider in Washington, DC, said that 30 percent of their patients reported fetal anomalies last year and, so far in 2024, they’re seeing a 30 percent increase over that baseline.
DuPont doesn’t turn anyone away who walks in their doors, Oza said, but that means “we are hemorrhaging money” and may be forced to close. Since July 1, DuPont has lost more than $80,000 in discounted care to provide abortions for people in the building, she said. DuPont has a new nonprofit arm, the Lavender Fund, that accepts donations to try to help offset its operating losses, a step Oza said was necessary “if we want to keep our clinic doors open.”
Before Dobbs, many pregnant patients with life-limiting fetal diagnoses—that is, impairments that mean the baby will be stillborn or only survive for a few hours—would have been able to receive a dilation and evacuation abortion in their local hospital. Women who got such diagnoses later in pregnancy, like after an anatomy scan, would typically have labor induced. Health insurance, if they had it, would usually cover either procedure.
Now, these patients are increasingly traveling to independent clinics like DuPont. Independent clinics—that is, non–Planned Parenthood providers—provide the vast majority of later abortions: Of clinics providing care after 22 weeks, 86 percent are independent; after 26 weeks, it’s 100 percent indies. Later abortion patients are either paying out of pocket or trying to get assistance from abortion funds to help them afford second- and third-trimester abortions, the most expensive procedures that are done over two or three days and often require hotel stays.
Independent clinics and funds are caring for this small but growing universe of patients on top of their typical clients, the majority of whom are receiving first-trimester abortions, at a time when funds are already facing a financial crisis due to cuts from the National Abortion Federation hotline fund and the Planned Parenthood Justice Fund. As of July 1, the groups said patient grants would be cut from up to 50 percent of procedure cost down to a maximum of 30 percent. Each NAF member clinic now also has a monthly cap, meaning some patients may not even get 30 percent. Dingus said a 16-year-old Illinois caller who needed $16,000 received just $600 from NAF. These drastic funding gaps are less likely to hit Planned Parenthood affiliates, because they typically don’t provide later abortion care.
Diane Horvath, cofounder and chief medical officer of Partners in Abortion Care, an all-trimester clinic in Maryland, said the clinic has always seen patients with fetal indications, but the numbers have increased since Florida’s six-week ban took effect in May. Patients who get early prenatal testing could receive a diagnosis of a life-limiting fetal condition at 13 or 14 weeks, but abortion is banned before that point across the Southeast. While some state laws do have exceptions for fetal anomalies, there has to be a provider at a hospital willing to perform the abortion, and Horvath said many are scared by the threat of losing their medical license or facing criminal charges.
“Even if they get [testing] at 10 weeks, by the time they could go up to North Carolina,” which bans abortions after 12 weeks, “there may not be an appointment available for them,” Horvath said.
“When people are forced to delay care, they could go from a same-day procedure to a two-day procedure, or from a two-day procedure to a three-day procedure,” Oza said. “That’s not how abortion care should be provided. It’s really a shame.”
Abortion funding cuts are affecting anyone across the country who needs help paying for an abortion, including if the pregnancy was wanted. As a result, people are scrambling to find money and then seeking care later in pregnancy, said Megan Kovacs, board member of Northwest Abortion Access Fund, which focuses on Washington, Oregon, Idaho, and Alaska. Kovacs said NWAAF had budgeted $1.5 million just for later abortions in 2024, but recently had to allocate another $825,000 to make it through the end of the year—that $2.3 million for later care is up from $1.1 million budgeted in 2023, and $702,000 in 2022. Still, she said the fund hasn’t noticed an increase in people disclosing fetal anomalies.
There are more mundane reasons people seek later care. Horvath said she recently provided an abortion to a woman whose OB’s office closed mid-pregnancy. The woman had to wait a few weeks to get into another practice, and her new doctor told her the fetus was unlikely to survive. “In that time, [an abortion] went from being a procedure she might have been able to get in her home state or closer to home, to something that she could only have in five clinics across the country,” Horvath said.
On top of these patients with anomalies, Horvath said, “there’s a giant chunk of people that have been trying to get an abortion for sometimes months, and now find themselves needing an abortion that’s gonna cost them a lot more money, take a lot more time, more childcare, more travel.” That’s more money abortion funds don’t have, and it’s a vicious circle that’s slamming clinic budgets, too.
Before the NAF cuts, Horvath said patients might show up and be missing 5–10 percent of their procedure fee. Now, they’re short 30–50 percent of the balance. Partners sees six to eight later abortion patients per week, and the shortfalls add up fast. Horvath told Rewire News Group that the clinic discounted nearly $15,000 in the first week of August alone.
Oza said this gap amounts to thousands of dollars: specifically, DuPont lost an average of $1,800 for every patient it’s served since July.
Popular
“swipe left below to view more authors”Swipe →
Current Issue
Amid this perfect storm slamming abortion providers and funds, yet another hit came on September 1: The nonprofit group Resources for Abortion Delivery is sunsetting a clinic-facing program called The Access Fund (TAF), which helped cover the cost of abortions up to 12 weeks for low-income people traveling from states with bans. TAF funds went to clinics in Illinois, New Mexico, Kansas, Georgia, and Florida, which have been considered “receiving states” for traveling patients.
Qudsiyyah Shariyf, deputy director of the Chicago Abortion Fund, said CAF estimated that the loss of TAF funding for clinics would represent “at least a $1 million hole nationally” each month, and noted that the majority of TAF-funded patients were getting care in Illinois. The Nation contacted Resources for Abortion Delivery to confirm the monthly budget and for comment about why TAF was ending; the group said it does not respond to press requests, as “a matter of long-standing organization policy.”
Any change in the funding ecosystem affects resources available for people across the country. When informed of TAF assistance ending, Dingus said, “I feel like you just punched me in the stomach because that’s so much money and so many people’s abortion care. It just feels like everything keeps getting squeezed.”
There is a program designed to help independent clinics, but it’s also struggling to keep up with what providers need, said Nikki Madsen, co–executive director of Abortion Care Network, a national member organization dedicated to supporting independent clinics. Since 2020, ACN has operated the Keep Our Clinics program, which fundraises for providers who lack the name recognition of affiliated clinics or hospitals, and members can apply for grants to cover equipment and supplies, rent, staffing, legal fees, and more.
Madsen said that member clinics have made $2 million in requests this year, but ACN expects that number to hit $4.5 million by the end of 2024. Madsen said Keep Our Clinics has only raised $750,000 so far. By comparison, the program raised and distributed more than $3 million in 2023 and nearly $5 million in 2022—and neither amount met the total need.
Some of the requests are coming from clinics in states where abortion is still legal, while others are from providers in places like Florida, where there’s a six-week ban in effect, though it could get overturned by a ballot measure in November. (She said there are 71 independent clinics in states with bans providing ultrasounds, miscarriage management, and abortion aftercare; 36 of them are in Florida alone.)
Independent clinics are critical “to all abortion care in America, but particularly care in the second trimester and beyond,” Madsen said, adding, “Truly, we cannot afford to lose any more clinics.” She said keeping them open “needs to be both a philanthropy and political priority.”
Kovacs said NWAAF was able to increase its budget for later care in part because it received an influx of institutional support since Dobbs, including $1 million from the state of Oregon, plus grants from the city of Portland and King County in Seattle. Other funds have also received such state and local grants, but it’s often not enough to meet the demand.
A collective of more than 30 abortion funds published an open letter in The Nation in August saying that national reproductive rights groups are directing gargantuan amounts of money to “vague, multiyear electoral strategies” rather than supporting people who need abortions now—and, in fact, cutting support to those people. Of the $100 million legislative campaign called Abortion Access Now, Horvath said, “I really hope that we are able to capitalize upon that. But, God, that would have paid for a lot of abortions—and, in a time when people are in crisis.”
To reduce the number of people traveling out of state, Congress needs to pass federal abortion protections. But clinics and funds say there are more immediate steps the Biden-Harris administration—or a future Harris-Walz one—could take.
The White House could provide federal funding for out-of-state abortion travel like it’s doing for military members, declaring a reproductive health emergency if necessary. Funding travel rather than procedure costs gets around the federal Hyde Amendment,


